Prognostic Modelling & Clinical Tools
Turning risk into a number a patient can use.
We build risk models that answer the questions patients actually ask, then turn them into calculators and apps for the clinic. The method is the same each time, careful development, external validation, and honest calibration. Only the question changes with the patient’s stage.
Epilepsy is a dynamic disease.
Risk is not a fixed label. After a brain insult, most seizure risk concentrates in the first year or two, then falls as a patient stays seizure-free. What people really want to know is their chance of a seizure in the next year, not an abstract ten-year figure. That shorter horizon is where the risk sits, where calculators are most accurate, and where decisions about driving, work, and treatment are actually made.
A tumour, then surgery
A patient develops epilepsy from a brain tumour, then has successful surgery. Is the epilepsy gone? Their risk, and even their diagnosis, may no longer be the same.
A seizure-free year
Someone has a single seizure after a stroke, then stays seizure-free for a year. Their risk of another seizure falls sharply. Do they still have epilepsy, and do they still need treatment?
These are not just calculations. They are deeper questions about what epilepsy is, and how we should quantify and talk about risk.
A model for each question along the journey.
SeLECT
Will epilepsy develop after a stroke or brain injury?
WAMS
Can antiseizure medication be safely withdrawn, and when?
COSY
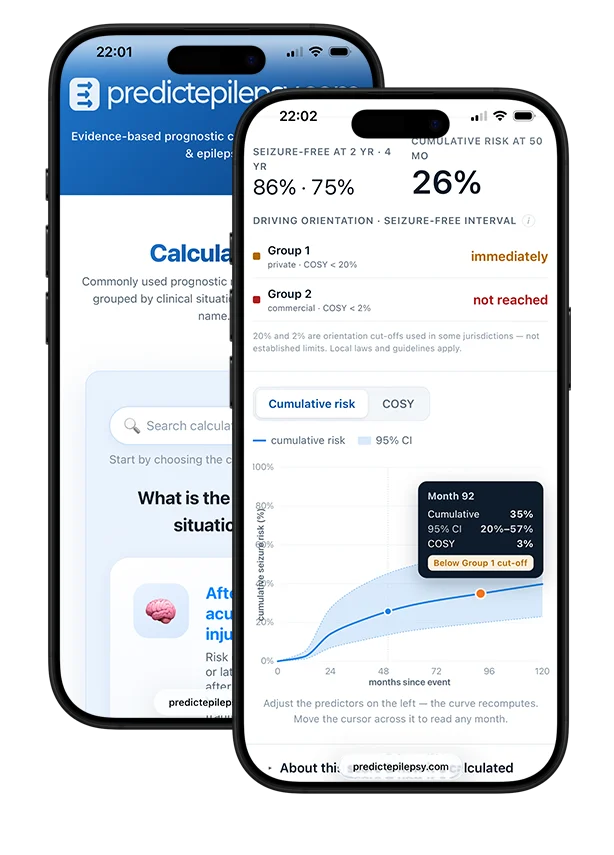
What is the chance of a seizure this year, for driving and work?
PEARLproof of concept
What is the malformation risk on a given medication?
Where our models become tools.
predictepilepsy.com is the home for these models, and other groups’ best models too, organised by the clinical question in front of you. Pick the situation, find the validated model, and get the number at the point of care. It is how our research reaches the bedside.
Which models can you trust?
Not every published risk model is reliable. We are building a framework to assess prognostic model quality, so clinicians can tell at a glance which tools are validated, calibrated, and safe to act on. This work is ongoing.
Our work on this topic, in the literature.
Timing of medication withdrawal after epilepsy surgery (WAMS)
Showed that when tapering begins matters, starting earlier than two years after surgery raised relapse risk, while waiting longer added no protection.
Epilepsy as a dynamic disease
Argued that seizure risk is short-term and moving, not a fixed 10-year label, and that near-term tools like COSY better match the decisions patients face.
Driving in people with seizures and epilepsy
Set out how individual seizure risk, expressed as the chance of a seizure in the next year, can inform fairer driving rules.
Prognostic models for seizures after stroke, tumours and TBI
A practical review of the risk models available across acquired epilepsies, and how to use them.
Mortality and epilepsy risk by acute seizure type (SeLECT 2.0)
Refined post-stroke epilepsy prediction and turned it into the updated SeLECT 2.0 model.
Predictive models for medication withdrawal after surgery (WAMS)
Built a validated model that gives individual relapse risk when considering stopping medication after epilepsy surgery.
Prognostic model of swallowing recovery after stroke
The same method beyond epilepsy, predicting who will regain swallowing after stroke to guide feeding decisions.
The SeLECT score for post-stroke epilepsy
The first validated model to predict late seizures after ischaemic stroke, from five routine variables.